Anterior Cruciate Ligament Injuries
The Knee Joint
The knee, which is the largest joint in the body, is considered a "hinged" joint since it is designed to allow the knee to flex (bend) and extend (straighten). The knee is formed by the femur (thigh bone), tibia (shin bone) and patella (kneecap). Each bone is covered with a layer of smooth cartilage, called articular cartilage.
The knee maintains its stability through a series of ligaments that act like rubber bands to allow motion while maintaining proper orientation of the bones. Both the anterior cruciate ligament, or ACL, and the posterior cruciate ligament (PCL) stabilise the knee. The ACL and PCL cross each other in the centre of the knee.
The ACL is tightest when the leg is straight, and the PCL is tightest when the leg is flexed. The ACL, which runs from the front of the tibia to the back of the femur, prevents the tibia from gliding forward. The PCL prevents the tibia from gliding backward.
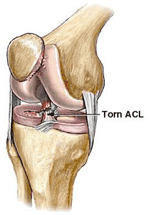
Anterior Cruciate Ligament Tears
The demands placed on the knee sometime exceed its limits. One common cause of ACL tears is rotating the leg inward while the rest of the body is turning outward. ACL injuries also may occur when the knee is turned outward while the upper leg is turning inward. This is most commonly seen in athletes as they change direction.
Diagnosis
History and physical examination are important to diagnosing an ACL injury. Explaining to your doctor or physiotherapist what movement caused your injury helps determine which part of your knee was damaged. It is common to hear or feel a “pop” at the time of injury. An X-ray may be ordered to rule out other problems.
Magnetic Resonance Imaging (MRI), may be used to get a detailed picture not often available through other testing. MRI can show changes in cartilage, tissue and bone structure resulting from injury. However, the diagnosis of ACL tear is usually made clinically by your doctor or physiotherapist.
Management
If you have suffered an ACL injury, treatment depends on many factors, including your lifestyle, work, sport and age. Your expectations for knee function or performance may play a role in determining whether reconstruction is needed. With an ACL tear, your knee is usually unstable. This instability may cause your knee to "give way" or feel unstable which will significantly influence knee function. If physiotherapy and the possibly the use of a special ACL brace do not improve the stability of the joint, your doctor may recommend surgical reconstruction. Your Sports physician will also consider whether there are additional knee injuries which make surgery necessary, such as a meniscal tear and discuss fully your options of treatment.
Physiotherapy
Whether you end up choosing surgery or conservative management, physiotherapy has an important role to play. In the early stages, your physio would help to reduce swelling, improve range of motion and minimise loss of muscle (particularly quadriceps). In later stages or post operatively, physiotherapists assist with rehabilitation, strengthening and functional return to activities.
Surgery
If ACL reconstruction is indicated, the surgeon will use the arthroscope to assist in this procedure through very small incisions.
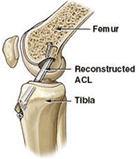
Reconstruction usually involves replacing the damaged ligament with a tendon graft. The graft is usually obtained either from the central third of your patellar tendon, or from a portion of your hamstring tendons. The graft will be placed in your knee in the same location as your natural ACL.
Resuming Activity
A specific exercise program recommended by your surgeon should be started after surgery. The exercises and physiotherapy are designed to re-establish range of motion and strength after ACL reconstruction. Return to pivoting and contact sports usually takes at least 6 months.



02 9231 0102
Park House Level 3, 187 Macquarie St Sydney NSW 2000
Park House Level 3
187 Macquarie St
Sydney NSW 2000
187 Macquarie St
Sydney NSW 2000